
Doctors and emergency medicine specialists across North America and beyond are increasingly warning the public about a disturbing and physically debilitating condition linked to chronic cannabis use.
Known medically as Cannabis Hyperemesis Syndrome (CHS) and colloquially as “scromiting” (a blend of screaming and vomiting).
This syndrome has become a growing reason people, especially young adults, are seeking urgent medical care. What may sound like an internet meme is in fact a severe and painful medical condition recognized by clinicians, public health authorities, and global health organizations.
In late 2025, the World Health Organization (WHO) formally added CHS to its global diagnostic classifications, giving it a specific code that will help doctors track and better understand its prevalence. This step was also adopted in the United States by the Centers for Disease Control and Prevention (CDC).
What Is Cannabis Hyperemesis Syndrome (CHS)?
Cannabis Hyperemesis Syndrome is a gastrointestinal disorder associated with frequent and long-term cannabis use.
It causes recurrent, severe nausea, intense abdominal pain, and repeated vomiting, often lasting hours to days — symptoms that can be so overwhelming that patients literally scream during episodes, hence the nickname scromiting.
In CHS, symptoms typically begin within about 24 hours after cannabis use and can continue until the underlying cause is addressed.
People experiencing CHS often report experiencing multiple episodes in a single year, and many have multiple emergency department visits before a correct diagnosis is made.
Why Does CHS Happen?
Although researchers are still investigating the exact cause, CHS appears to result from the chronic overstimulation of the body’s endocannabinoid system, which plays an important role in regulating nausea, digestion, and the body’s stress responses.
Cannabis contains compounds called cannabinoids — particularly THC (delta-9-tetrahydrocannabinol) — that interact with cannabinoid receptors in both the brain and the gastrointestinal tract.

While acute cannabis use can reduce nausea, long-term exposure seems to produce paradoxical effects in some individuals, triggering the very symptoms it sometimes temporarily relieves.
Some scientists also note that variations in cannabis potency, cannabinoid composition, and individual biological differences may contribute to why only a minority of users develop CHS.
Many questions remain about genetics and predisposition, but current evidence shows that heavy, frequent, and long-term use — especially daily use over a year or more — increases risk.
The Three Phases of CHS
Clinicians and researchers describe CHS as progressing through three distinct phases, each with different symptoms:
1. Prodromal Phase
This early stage can last for months or even years before full symptoms appear. It is characterized by:
Persistent or recurring nausea
Mild to moderate abdominal discomfort
Morning queasiness
Occasional fear of vomiting
People in this phase may often use more cannabis thinking it will relieve their nausea, which can unfortunately accelerate the progression toward full CHS.
2. Hyperemetic Phase
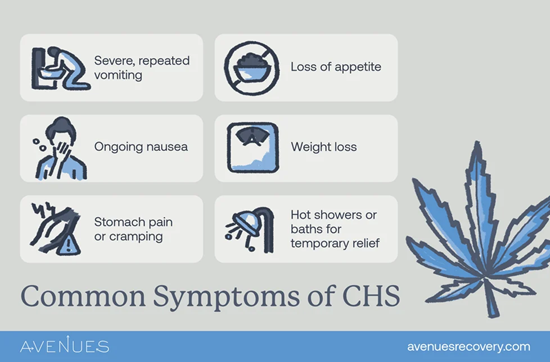
This is the acute and most dramatic phase of CHS. Symptoms include:
Severe, uncontrolled nausea
Intense and recurrent vomiting
Cramp-like abdominal pain

Reduced appetite and weight loss
Dehydration from fluid loss
One particularly unusual and well-documented aspect is that many sufferers find temporary relief from symptoms by taking hot showers or baths, often for extended periods. This behavior is so common that clinicians consider it a helpful diagnostic clue.
3. Recovery Phase
If cannabis use stops entirely, symptoms begin to resolve and may disappear over days to weeks. However, if cannabis is used again, even after a period of abstinence, symptoms often return.
Why Is CHS Often Misdiagnosed?
Because CHS symptoms — nausea, vomiting, abdominal pain — overlap with many other gastrointestinal disorders, it is frequently misdiagnosed initially as food poisoning, cyclic vomiting syndrome, gastritis, or other stomach conditions.
Before WHO’s formal diagnostic code, the lack of a specific classification meant that many CHS cases were simply labeled as generic vomiting disorders.
Some patients report lasting months or years of repeated medical evaluations before a correct CHS diagnosis is made.
How Serious Can CHS Be?
CHS is more than an unpleasant side effect — it can lead to significant medical complications if not addressed:
Severe dehydration
Electrolyte imbalances
Weight loss and malnutrition
Tooth enamel erosion from frequent vomiting
Kidney injury
In rare cases, aspiration pneumonia or cardiovascular strain
For these reasons, people experiencing severe symptoms are often treated in emergency departments with intravenous fluids and supportive care.
How Is CHS Treated?
At present, there is no approved pharmaceutical cure for CHS. Doctors focus on managing symptoms and preventing complications. Some of the approaches used include:
IV fluids for dehydration
Traditional anti-nausea medications (though they are often less effective in CHS)
Topical capsaicin cream, applied to the abdominal area
In some cases, medications such as antipsychotics (e.g., haloperidol) have provided relief in controlled settings
Continuous hot showers or baths for temporary symptom reduction
However, the only known way to stop CHS permanently is complete cessation of cannabis use. Continued use almost always leads to further episodes, even if symptoms temporarily subside.
Who Is at Risk?
Certain patterns of cannabis use are consistently associated with higher risk:
Daily or near-daily cannabis use
Long-term use for a year or more
Frequent use of high-THC products
Starting regular cannabis use at a young age

Emergency department data suggest that CHS cases have increased over the past decade as cannabis use has become more common and products have become stronger, particularly among young adults aged roughly 18–34.
Why Is CHS Increasing?
Although chronic cannabis use has long been common in some populations, recent research shows a marked rise in CHS diagnoses and emergency room visits over the last decade.
A major national analysis found that cases of CHS increased several-fold in emergency departments from 2016 through 2022, particularly in young adults and in regions where cannabis access and potency have grown.
Part of the observed increase likely reflects both greater recognition by clinicians and higher overall use of cannabis products, especially high-potency tinctures, edibles, and concentrates that deliver large amounts of THC.
Public Health Implications
With CHS now formally recognized by international health authorities, clinicians have better tools to diagnose and code cases accurately. This will improve data collection, surveillance, and research, ultimately helping healthcare systems respond more effectively.
Education for both healthcare providers and cannabis users is critical, because many patients assume their symptoms are unrelated to cannabis or are something less serious.
As medical awareness grows, earlier identification and counseling may prevent repeated hospital visits and long-term health consequences.
Final Takeaways
Cannabis Hyperemesis Syndrome (CHS), sometimes referred to as scromiting, is a real and serious condition linked to frequent, long-term cannabis use.
It causes cycles of intense nausea and vomiting, often accompanied by abdominal pain and unusual symptom-relief behaviors like prolonged hot showers.
While symptoms can be brutal and frightening, the best evidence shows that completely stopping cannabis use is the only reliable way to stop CHS and prevent its return